Medical Simulation is a learning technique and not just a technology. Understanding some of the learning theories behind healthcare simulation may help team members with limited experience in education understand the reason for the success of sim as a teaching methodology. Clinical simulation is based on the adult learning theory, aka Andragogy Theory, but also calls upon Transformative Learning as described by Mezirow and Experiential Learning by Kolb.
Today’s article was guest authored by Kim Baily PhD, MSN, RN, CNE, previous Simulation Coordinator for Los Angeles Harbor College and Director of Nursing for El Camino College. Over the past 16 years Kim has developed and implemented several college simulation programs and previously chaired the Southern California Simulation Collaborative.
Here Dr. Baily helps us to better understand the key learning theories necessary for Simulation in Healthcare, which will be a useful consideration for Sim Techs or clinical educators new to Sim:
Andragogy Learning Theory, How Adults Learn
In the 1970s, Malcolm Knowles listed 6 reasons that adults learn differently from children:
- Need for Knowledge: Adults need to know “why” they should learn.
- Motivation: Adults are driven by internal motives. They will learn if they want to learn. For instance, a compelling answer to the “what’s-in-it-for-me” question is a powerful internal motivation.
- Willingness: For adults, the willingness or readiness to learn comes from perceiving the relevance of the knowledge. They want to know how learning will help them better their lives, and they learn best when they know that the knowledge has immediate value for them.
- Foundation or Experience: Adults bring with them rich reserves of experiences that form the foundation of their learning. They analyze, rationalize, synthesize, and develop new ideas or tweak old ones through the filter of their experiences. As an instructional designer, you should tap into their well of experiences to help them make connections, perceive relevance, and derive inspiration.
- Self-Direction: Adults are self-directed individuals who want to take charge of the learning journey. They are independent beings who want to feel in control.
- Orientation to Learning: Adults learn best when they “do.” They find relevance in task-oriented learning, which they can align with their workplace realities. Besides, task-oriented learning exercises their problem-solving ability that in turn, gives them the confidence that they can conquer their challenges with their newly-acquired knowledge.
Adults consider past experiences to decide whether something is worth learning. To teach adults effectively, instructors must be able to feed into what learners already know. Like piggy-backing off old concepts, new concepts must minimize data clashes with an existing knowledge base. Instructors must skillfully integrate new learning into learner’s lived experience to become an active part of their thought process.
Important to consider, is that if adults do not find a relevance they will lose interest. In an age of cell phones, the good news about simulation is that it is directly interactive and experiential!
Transformative Learning
“Learning is understood as a process of using a prior interpretation to construe a new or revised interpretation of the meaning of one’s experience in order to guide future action” (Mezirow, 1996, p. 162). Some educators call this the aha moment when an insight changed long held beliefs. For example, learning styles has been a long held view about the way people learn. In fact, many educators still believe this despite a total lack of scientific evidence to support this theory. Check out the HealthySim article published June 2018 entitled “Are Learning Styles Debunked? What We Need to Know for Healthcare Simulation” and see if you have an “Aha!” moment about the fallacy of learning styles.
Mezirow described 10 phases in Transformational Learning:
- A disorienting dilemma.
- Self-examination with feelings of guilt or shame.
- A critical assessment of assumptions.
- Recognition that one’s discontent and process of transformation are shared and that others have negotiated a similar change.
- Exploration of options for new roles, relationships, and actions.
- Planning of a course of action.
- Acquisition of knowledge and skills for implementing one’s plans.
- Provisionally trying out new roles.
- Building of competence and self-confidence in new roles and relationships.
- A reintegration into one’s life on the basis of conditions dictated by one’s new perspective.
Although the phases above may seem overly complex, they often occur in simulation. For example, during a code simulation a learner may realize that their entire focus on chest compressions or applying patches has caused them to miss a critical change in cardiac rhythm. Participants learn about their own responses and errors and will then plan to change their responses or perspectives. Allowing learners to reflect upon their actions during debriefing will lead the learners to transform future behaviors.
Experiential Learning (Kolb)
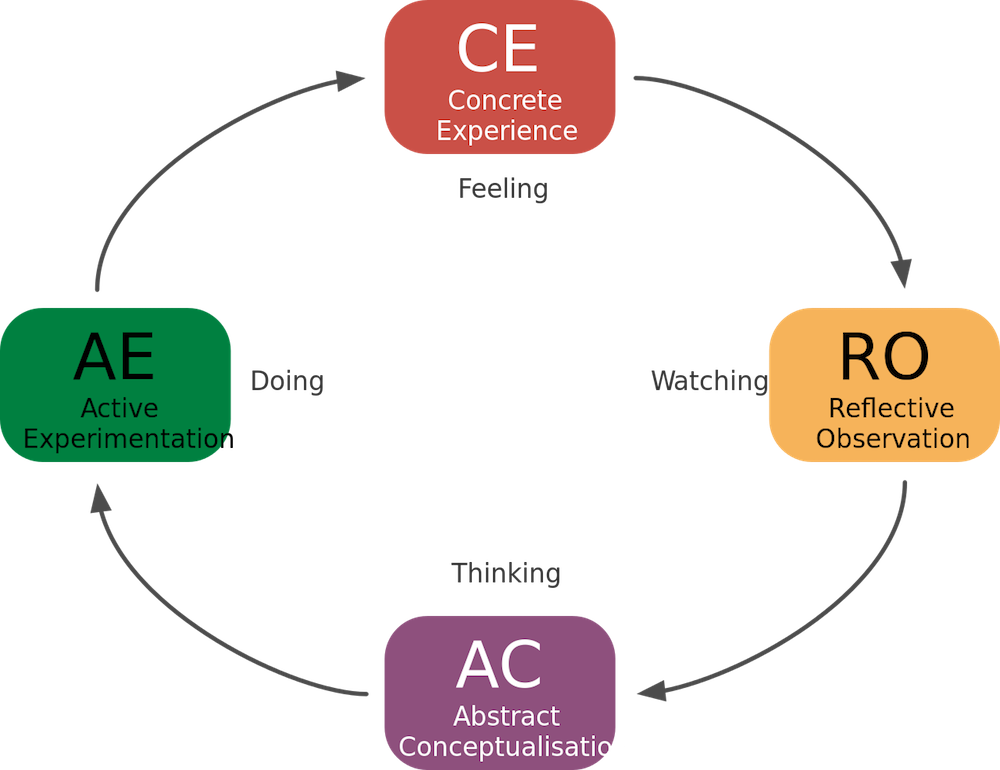
Experiential Learning Theory is a four-stage cyclical theory that involves a holistic perspective that combines experience, perception, cognition, and behavior.
- Concrete experience (or “DO”). The learner actively experiences an activity such as a lab session or field work. Medical simulation creates kinesthetic learning (learning by physical actions). Simulation may evoke strong emotional responses that reveal cause-effect relationships which will be remembered by the learners.
- Reflective observation (or “OBSERVE”). The learner consciously reflects back on that experience. Debriefing allows time for learners to reflect and analyze their own behaviors.
- Abstract conceptualization (or “THINK”). The learner attempts to conceptualize a theory or model of what is observed. Simulations allow learners to think critically about a given situation. They will formulate concepts and plan behaviors for future events.
- Active experimentation (or “PLAN”). The learner is trying to plan how to test a model or theory or plan for a forthcoming experience. Role-playing activities, internships, and other hands-on tasks let learners apply the learning and thus truly “learn by doing.” Active experimentation leads to concrete experiences, and the cycle of experiential learning resumes.
The debriefing phase of medical simulation is a key component of nursing simulation education. During this phase, learners should be guided (not lectured at) to reflect back on their own behaviors, determine their own concepts and whether they are correct or not and then plan changes for their future behaviors. Simulation is a terrific way to educate healthcare practitioners at all levels. Thank you if you play any role in simulation education! You make a difference to patient safety, one scenario at a time!
Learn more about Learning Theories for Medical Simulation!
Have a story to share with the global healthcare simulation community? Submit your simulation news and resources here!





